Bisection, Disjuncture, Aqueduct: Pancreas Divisum
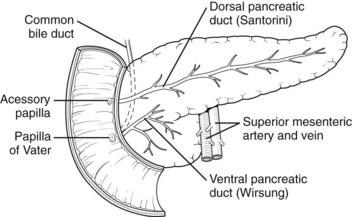
The conformable congenital anatomic malformation of the pancreas is Pancreas Divisum. Conventionally, the pancreas evolves from the fusion of the dorsal and the ventral pancreatic buds throughout the sixth week of gestation. The dorsal bud structures the head, tail and the body of the pancreas while the ventral bud configures the uncinate process besides the inferior portion of the head. The concurrence of this arrangement permits the amalgamation of the ductal schemata so the major pancreatic duct evacuates the pancreatic secretions into the duodenum through the major duodenal papilla. Comparatively 30% of entities delineate the traditional anatomical derivatives, where the proximal dorsal pancreatic duct prevails as the accessory pancreatic duct and expels through the minor duodenal papilla.
Disease Characteristics
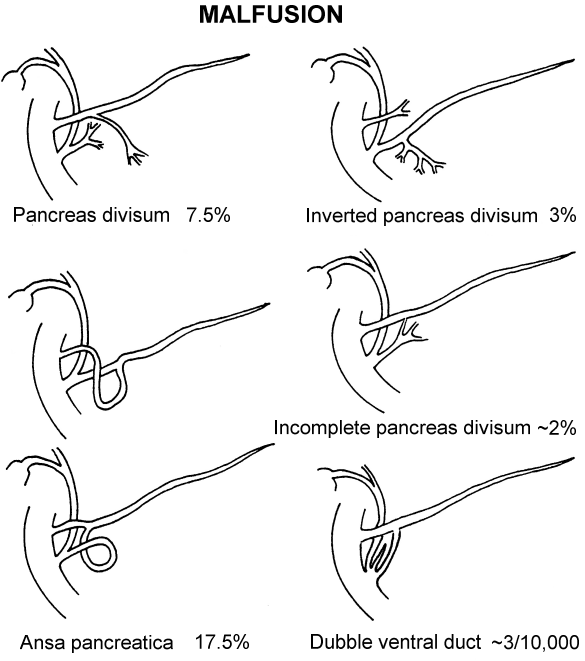
In pancreas divisum, the typical characteristic commingling of the dorsal and the ventral ductal complex disintegrates. Two definite channels are outlined wherefore the dorsal duct depletes the majority of the pancreas by virtue of the minor papilla and the ventral duct dissipates only the inferior portion of the head of the pancreas along the major papilla [1, 2]. The incomplete pancreas divisum is an uncommon anatomic modification which evinces a narrow, frequently defective conduit between the dorsal and ventral pancreatic duct where the bulk of the enzymatic/hormonal discharge ensues by the route of the smaller minor papilla. The prevalence of the pancreas divisum is to the scale of 5-10% of the recorded autopsies [3, 4]. Pancreas divisum, though existing as a congenital aberrance remains undetected until the fifth decade, then commences to be inherently demonstrative [5]. Pancreas divisum can be identified in the inexpressive individuals utilizing the cross –sectional imaging modalities. Pancreas divisum , when detected with idiopathic acute or recurrent pancreatitis, is clinically indicative. Pancreas divisum is associated with evolution of pancreatitis, as assessed in a retrospective study of endoscopic retrograde cholangio pancreatography (ERCP) [5] (Figure1). Though the global prevalence of pancreas divisum is analyzed at 3.6%, patients with obscure recurrent pancreatitis are recognized to have a sizeable association (25.6%). An obstructive pancreatopathy with the narrow minor papilla brings about the exudation of the greater part of the pancreas via the dorsal pancreatic duct and is the residuum of pancreatitis in pancreas divisum [5]. Anatomic derivatives and the normal architecture of the pancreas are described.
| Bajaji A* Histopathologist in A B Diagnostics, India *Corresponding author: Anubha Bajaji, Histopathologist in A.B. Diagnostics, | Review Article | |||
| Volume 3 Issue 1 | ||||
| Received Date: August 08, 2018 | ||||
| Published Date: August 24, 2018 |
Investigations
Pancreas divisum has been much elucidated in the last two decenniums on account of the utilization of cross sectional imaging with the Magnetic Resonance Imaging (MRI) and Magnetic Resonance Cholangio Pancreatography (MRCP). MRCP carries an identical diagnostic precision in the assessment of pancreas divisum. Moreover, secretin enhanced MRCP (S-MRCP) exposes the pancreas divisum by provoking a bicarbonate rich fluid secretion into the pancreatic ducts thereby ameliorating the anatomic characteristics [6]. Secretin reinforced MRCP emphasizes the diagnosis of the malfeasance with a sensitivity of 86% in contrast to 52 % on a standard MRCP, thus establishing the interpretative non invasive imaging [7].
Therapeutic Interventions
for patients with recurrent acute pancreatitis (RAP) and pancreas divisum requires the alleviation of the contingent obstructive pancreatopathy engendered by a stenotic minor papilla. Surgical mediation with a minor papilla sphincteroplasty has been implemented with a favourable outcome. Endoscopic therapy is an approbated option with a minimal transgression. Endotherapy for pancreas divisum may incorporate a dorsal duct pancreatic stent installation [8] or commonly an endoscopic minor papillotomy. Aforesaid endoscopic therapies demonstrate clinical alleviation in patients with recurrent acute pancreatitis complemented with pancreas divisum. Candidates enduring chronic pancreatitis subsidiary to pancreas divisum or abdominal pain in the absence of pancreatitis may not be suited to analogous mediations [9]. Interval endosonography with chronic pancreatitis are reduced in individuals with recurrent acute pancreatitis consequent to pancreas divisum thereby implying that an early intercession with endotherapy may be justified. Post ERCP pancreatitis upsurges with dorsal duct cannulations and endoscopic minor papillotomy (Figure 2).
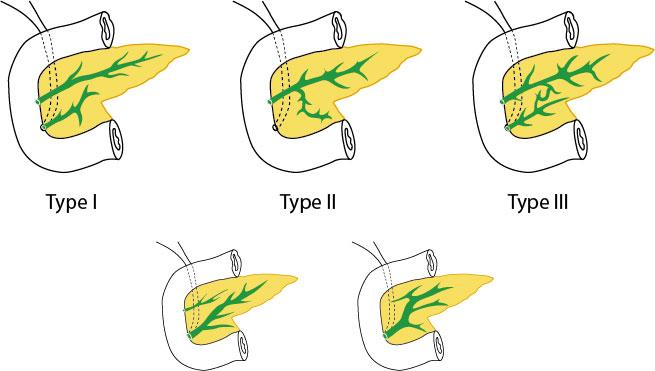
Pancreas divisum can terminate in a Santorinicoele as enunciated by the cystic dilatation of the distal dorsal duct (santorini’s duct) and an abutting minor papillae Three subdivisions are acknowledged:
- Type I (Classic): The coalition between dorsal and ventral pancreatic ducts is absent. It manifests in 70% cases.
- Type II (Absent ventral duct): The minor papillae depletes the entire pancreas although the major papilla and exhausts the bile duct. The accounted frequency is 20-25%.
- Type III (Functional): The conduit between dorsal and ventral pancreatic ducts is filamentous or insufficient. Connotes in 5-6% of the discovered malformations.
Isolated Therapeutic Endotherapy
Recurrent acute pancreatitis coexists with pancreas divisum. Deliberation concerning the exact origin of pancreatitis states that it is either antecedent to the anatomical arrangement or subsidiary to the coexistent comorbidities. The impact of pancreas divisum on the furtherance of chronic pancreatitis is assessed by MRCP and ERCP. Pancreas divisum neither determines nor transforms the age of inception of chronic pancreatitis (CP). In spite of the pancreas divisum, aberrations of the ventral duct persist (75% cases prevail with history of alcohol abuse and 72% patients subsist with the lack of alcohol misuse).
Genetic Mutations
Genetic mutations are recognized with a greater prevalence in pancreatitis concomitant with pancreas divisum SPINK -1 mutation persist with recurrent acute pancreatitis coexistent with pancreas divisum (41.6%). SPINK -1 is identically established in candidates with the absence of pancreas divisum who present with idiopathic chronic pancreatitis (43.3%) and idiopathic recurrent acute pancreatitis (35.6%), thus implying that the mutation and not the congenital malfeasance is probably advancing the pancreatitis. Besides, deviation of the CFTR gene is elaborated in patients exhibiting pancreas divisum with pancreatitis. Along with the escalated viscosity of the pancreatic fluid, CFTR malfunction induces a disproportionate host inflammatory reaction to further constrict the perpetually narrow pancreatic duct orifice in the pancreas divisum, thus activating the pancreatitis. Nevertheless, CFTR mutations and pancreas divisum may coincide without instigating the pancreatitis or altering the associated genetic perceptivity [10]. Adult onset pancreatic disease can be unearthed with complete gene sequencing, thus expediting the detection of high risk mutations.
Discussion
Pancreas divisum is an embryonic deficiency in the amalgamation of dorsal and ventral pancreatic buds. The disorder in the Caucasians is assessed to be from 9.3- 10.8% when delineated by the MRCP and 5-6% in relation to the ERCP. Usually the minor papillae are miniscule but discharge the pancreatic juice maximally in the pancreas divisum. Thus an upsurge in the flow precipitated by a fatty diet in alliance with the papillary stenosis may augment the dorsal duct pressure and delineate obstructive pancreatitis. Endoscopic or surgical sphincterotomy of the accessory papilla to diminish the pressure of the pancreatic duct in clinical scenarios has been contemplated. Contradictions are on account of fact that the pancreas divisum is not prevalent enough in idiopathic pancreatitis (IP). Besides, pancreatitis tends to exist in the ventral duct system of the pancreas divisum [11]. Clinical manifestations are depicted in fewer than 5% patients of pancreas divisum [11]. Hence the employment of endotherapy in candidates of idiopathic pancreatitis with pancreas divisum is dubious, though endotherapy has assisted in pain relief in addition to a declining incidence of recurrent pancreatitis and hospitalization. However the affinity of pancreas divisum with idiopathic pancreatitis is inconclusive as elaborated: i) The uncertain diagnosis of the pancreas divisum, ii) the benevolent clinical progression in synchronous idiopathic pancreatitis and pancreas divisum with consequent negligible endotherapy iii) the lack of adequate data to rationalize the application of specified invasive measures [11]. An ultrasound a computerized tomography (CT) scan and conventional magnetic resonance (MR) imaging are regularly employed in the evaluating patients with pancreatic symptoms. Despite the convenience in the interpretation of the pancreatic parenchyma, the exposure of duct peculiarities of the pancreas divisum is restricted. A lobular architecture of the pancreas, a homogenous expansion of the pancreatic head or a fat cleft disconnecting the dorsal and ventral pancreatic moieties are displayed on CT. However these adjunctive features are of slight relevance. ERCP is the prevalent, contemporary approach to the diagnosis of pancreas divisum. It comprises of the cannulation of the major papilla subsequent to the injection the contrast medium into the short, thin, blind ended ventral duct which characteristically has no connection with the dorsal duct. The minor papilla is then cannulated and the communion betwixt the dorsal duct and the main pancreatic duct is illustrated. The ERCP is often misrepresented, as in a short ventral duct being elucidated as a pancreas divisum (a false pancreas divisum). Alternative pathologies ascribed are a fibrotic stricture in an alcohol induced pancreatitis or a psuedocyst in chronic pancreatitis, previous pancreatic trauma, partial pancreatectomy or a tumour. Severe pancreatitis is attributed to the cannulation of the minor papillae (2%). MRCP is a modernistic imaging modality which permits a non- invasive multiplanar resolution of the biliary tree and the pancreatic ducts excluding a contrast medium. Anatomical appraisal of the pancreatic ducts is recommended as it reduces iatrogenic complications secondary to a failed cannulation of the dorsal duct [12]. The fast magnetic resonance automation applying the phased array coil has ameliorated the image resolution and diagnostic precision. Since the determination of pancreas divisum is challenging, the occurrence of associated pancreatitis is miscalculated (Figure 3). Acute pancreatitis in young patients, with absent cholelithiasis is adjunctive to chronic, excessive alcohol intake and hyperlipidaemia. Infrequent and concomitant conditions such as pancreas divisum with acute pancreatitis are generally overlooked. Diagnostic methods such as ERCP, CT scan, and MRCP may not be universally or consistently accessible, along with a competent investigator to assimilate and conclude the diagnosis of pancreas divisum [12, 13].
Conclusion
Pancreas divisum is feasible source of acute pancreatitis in young adults generally misinterpreted as of alcoholic, hypertriglyceridemia or idiopathic aetiology. A precise determination of the malfeasance is pertinent to cogitate a dynamic, invasive therapeutic option such as sphincterotomy for a pancreas divisum with recurrent pancreatitis or incessant pain. The non-invasive and eminently interpretable MRCP is the preferential diagnostic approach to assess patients with pancreas divisum, an underreported stimulator of young acute pancreatitis which solicits cogent therapeutics.
References
-
Schoewolf G et al. (2015) Larsen’s human embryology 5th (Edn), Philadelphia PA, Elseiver.
-
Klein SD (2004) Pancreas divisum, evidence based review, part I pathophysiology Gastrointestinal Endosc 60: 419-425.
-
Kleitsch WP (1955) Anatomy of the pancreas: A study with special reference to the duct system ANA Arch Surg 71(6): 795-802.
-
Dawson W, Langman J (1961) An anatomical radiographic study of the pancreatic duct pattern in man Anat Rec 139: 59-68.
-
Cotton PB (1980) Congenital anomaly of pancreas divisum as a cause of obstructive pain and pancreatitis Gut 21(2): 105-114.
-
Matos C, Metens T, Devière J, Delhaye M, Le Moine O, et al. (2001) Pancreas divisum evaluation with secretin enhanced magnetic resonance cholangiopancreatogarphy Gastrointest Endosc 53(7): 728-733.
-
Rustagi T, Njei B (2014) Magnetic resonance cholangiopancreatography in the diagnosis of pancreas divisum; A systematic review with metanalysis. Pancreas 43(6):823-828.
-
Ertan A (2000) Long term results after endoscopic pancreatic stent placement without pancreatic papillotomy in acute recurrent pancreatitis due to pancreas divisum Gastrointest Endosc 52(9): 9-14.
-
Chacko LN, Chen YK, Shah RJ (2008) Clinical outcomes and non endoscopic interventions after mino papilla endotherapy in patients with symptomatic pancreas divisum. Gastrointest Endosc 68(4): 667-673.
-
Di Magno, Dimagno EP (2012) Pancreas divisum does not cause pancreatitis but associates with CFTR mutations Am J Gastroenterol 107(2): 318-320.
-
Fogel EL, Toth TG, Lehman GA, DiMagno MJ, DiMagno EP (2007) Does endoscopic therapy favourably affect the outcome of patients who have recurrent acute pancreatitis and pancreas divisum Pancreas 34(1): 21-45.
-
Leiver VH, van Hoe L, Vanbeckevoort D, Mermuys K, Steenbergen W (2006) MR Cholangiopancreatography Atlas with cross sectional Imaging Correlation Ist(Edn) Berlin Springer 136-149.
-
Dennis Kumral, John Baillie (2017) Pancreas Divisum : on life support but not quite dead JOP J of Pancreas Mar 30 18(2): 97-100.
- Management of Gallbladder Perforations: A Review
- From The Mouth to the Gut: The Oral Microbiome's Role in Promoting Gastrointestinal Disease
- Case Report: Intraductal Papillary Mucinous Neoplasm (IPMN) Complicated by Portal Vein Plaquing and Biliary Obstruction Mimicking Pancreatic Metastatic Malignancy
- Management of Non-Cirrhotic Portal Hypertension during Pregnancy: A Review
- Effectiveness of Omeprazole versus Pantoprazole for Symptomatic Relief of Gastro-Esophageal Reflux Disease (GERD)/ Acid Peptic Disease (APD): A Real-World Evidence (RWE) Study
- Case of Splenic Infarction; A Rare Presentation of Complicated Enteric Fever in a Pediatric Patient